
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
Advertisement
Scientific Reports volume 15, Article number: 265 (2025)
1537
Metrics details
Multiple artificial intelligence systems have been created to facilitate accurate and prompt histopathological diagnosis of tumors using hematoxylin-eosin-stained slides. We aimed to investigate whether weakly supervised deep learning can aid in glioma diagnosis. We analyzed 472 whole slide images (WSIs) from 226 patients in West China Hospital (WCH) and 1604 WSIs from 880 patients in The Cancer Genome Atlas (TCGA). We utilized the OpenSlide library to load WSIs, segmented them into small patches using the DeepZoom module, and then normalized the color using the Reinhard method. A weakly supervised deep learning model was developed using ResNet-50 combined with an attention mechanism. We investigated the performance of the model by calculating area under the curve (AUC) in a ten-fold cross-validation setting. Heatmap visualizations showed the prediction mechanism of the model. The results were promising, with high AUC values for differentiating grades of astrocytomas, oligodendrogliomas, all gliomas, and glioma types in the TCGA dataset (0.9419, 0.8659, 0.9904, and 0.9298, respectively), and in the WCH cohort (0.9048, 0.7423, 0.9510, and 0.7098, respectively). The model demonstrated a strong ability to infer IDH status in the TCGA dataset (AUC = 0.9488). The weakly supervised deep learning model proved to be an effective and reliable tool for neuropathological diagnosis, making it an attractive auxiliary tool.
An estimated 26,670 new cases of malignant tumors of the central nervous system (CNS) are expected to be diagnosed in the United States in 20221. Glioma is the most common primary malignant tumor in the CNS, with glioblastoma (GBM) accounting for approximately more than half of all glioma cases1. In terms of the 5-year survival rate, merely 6.9% of GBM patients have an opportunity to survive beyond five years, highlighting their high mortality1. Accumulating evidence demonstrates that precisely histopathological and molecular diagnosis of gliomas is a mainstay in developing effective anti-tumor regimes and predicting patient outcomes2. Thus, the 2021 fifth edition of the WHO classification of tumors of the CNS has updated the significant role of a variety of molecules in classifying CNS tumors, building upon the updated 2016 fourth edition2,3. For instance, the nomenclature for GBM, IDH-mutant, and WHO grade IV has been revised to astrocytoma, IDH-mutant, and WHO grade 4. Additionally, adult-type diffuse gliomas without an IDH mutation are now uniformly diagnosed as GBM, IDH-wildtype, and WHO grade 4, irrespective of their morphological characteristics2.
Although molecular diagnostics has become indispensable for classifying CNS tumors in the molecular era, it remains wedded to the traditional approaches of histology and immunohistochemistry. Both histological and molecular diagnostics require highly skilled pathologists with years of experience in manually handling and identifying tissue sections, making the diagnostic process labor-intensive, especially with a large patient population. Additionally, interobserver variability in diagnoses raises concerns about the consistency and precision for each patient4. In recent years, computational pathology, based on whole slide images generated by advanced digital slide scanners, has emerged as an effective method for enhancing the efficiency and accuracy of diagnoses for pathologists5,6. Moreover, deep learning algorithms, which integrate convolutional neural networks (CNNs) with prognosticators from the widely available WSIs, are capable of predicting time-to-event outcomes in various tumors7,8,9. Nonetheless, cross-institutional studies are needed to validate the accuracy and efficiency of artificial intelligence (AI) assisted pathological classification.
In terms of glioma research, a prominent study demonstrates that a deep learning model can assist pathologists in classifying the five histological subtypes of gliomas with a patient-level accuracy of 87.5%10. An earlier study employs a coarse-to-fine analysis strategy based on whole slide images (WSIs) and achieves an accuracy of 93.1% in distinguishing GBM and lower-grade gliomas10. Deep CNNs (DCNNs) can also automatically identify key histopathological tumor regions that correlate with GBM patient survival11. Several studies have leveraged deep learning to classify WHO grades, histological subtypes, and molecular status of gliomas with a relatively high accuracy12,13,14,15. However, most of these studies predominantly use supervised deep learning algorithms, which inherently require pathologists to annotate the regions of interest (ROIs) or pick image patches on WSIs. Subsequently, computer-aided algorithms are developed based on the selected ROIs for tumor classification. Due to the necessity of expert pathologist supervision, early models face limitations in real-world applications, as obtaining accurate WSI annotations from doctors is labor-intensive, and the robustness of diagnosis is compromised as the selected ROIs hardly encompass all the relevant information from the WSIs. Recently, weakly supervised deep learning models have been introduced to address these limitations16,17,18. The advantage of weakly supervised deep learning algorithms is their capability to operate with a single label per slide, thus eliminating the need for annotation at the ROI level by pathologists6,19. These novel methods appear to detect tumors and classify tumor subtypes with high accuracy6,19,20,21. Nevertheless, there is a scarcity of research employing weakly supervised deep-learning algorithms to identify glioma types, grades, and molecular markers.
In the current study, we evaluate the diagnostic accuracy of histopathological and molecular classification of gliomas on the TCGA dataset and West China Hospital (WCH) dataset with a well-established weakly supervised deep learning algorithm19. The clustering-constrained-attention multiple-instance learning (CLAM) model employs the self-attention mechanism to accurately classify whole slides19. Importantly, CLAM requires only slide- or patient-level labels for training and, without any input from pathologists, completes the fundamental yet onerous task of subtyping gliomas, including the discrimination of a key molecular marker. We propose that the weakly supervised deep learning model is a valuable addition to an integrated neuropathological diagnosis workflow, in line with the 5th edition of WHO CNS tumor classification.
A total of 226 patients with five glioma subtypes, including astrocytoma, anaplastic astrocytoma, oligodendroglioma, anaplastic oligodendroglioma, and glioblastoma (472 hematoxylin-eosin (HE) WSIs from 226 patients) were recruited from the West China Hospital. 880 patients with the same 5 subtypes (1604 HE WSIs from 880 patients) were enrolled from the TCGA. All demographic and clinical characteristics of the data in the present study are detailed in Table 1.
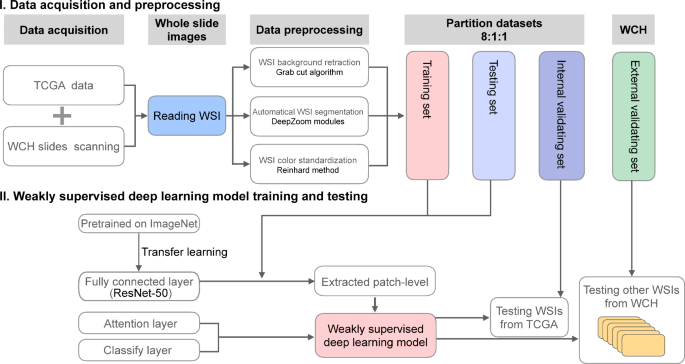
The workflow of the study, presented in Fig. 1, includes two main procedures: (I) Selecting and collecting WSIs of HE staining slides from the TCGA and WCH, and preprocessing them using a pipeline of approaches. We partitioned the TCGA WSIs into three subgroups: the training set, the testing set, and the internal validation set with a proportion of 8:1:1. The external validation set, used for testing diagnostic accuracy, included 472 HE WSIs from our institution. (II) Testing the diagnostic accuracy of the weakly supervised deep learning model. Representative HE images from the WCH show distinct morphological characteristics of each glioma subtype (Fig. 2a–f).
The workflow of the present study. The whole slide images (WSIs) of HE staining slides from the TCGA and WCH were collected and preprocessed through a pipeline of procedures, and then data were partitioned into three subgroups (I). Transfer learning was used to extract high-quality patch-level features, and then a weakly supervised deep learning model was generated and pretrained and tested employing the training dataset (II). Finally, the model was used to determine the final diagnosis and diagnostic accuracy was validated using the internal and external validation datasets, respectively (II).
Representative HE images of each subtype of gliomas of WCH. (a) Oligodendroglioma, IDH-mutant and 1p/19q codeletion, WHO grade 2. (b) Anaplastic Oligodendroglioma, IDH-mutant and 1p/19q codeletion, WHO grade 3. (c) Astrocytoma, IDH-mutant, WHO grade 2. (d) Anaplastic Astrocytoma, IDH-mutant, WHO grade 3. (e) Glioblastoma with morphology of WHO grade 3 astrocytoma, IDH-wildtype, WHO grade 4. (f) Glioblastoma with typical risk features of extremely dense cells and plenty of microvascular proliferation, IDH-wildtype, WHO grade 4. Magnification, 200X.
The original TCGA database comprises n = 1604 WSIs (Astrocytoma n = 346, Anaplastic astrocytoma n = 220, Oligodendroglioma n = 163, Anaplastic oligodendroglioma n = 115, Glioblastoma n = 760). We conducted ten-fold cross-validation to assess the reliability of the weakly supervised deep learning model across all diagnostic tasks. We plotted the receiver operating characteristic (ROC) curves and calculated their corresponding area under the curve (AUC), as depicted in Fig. 3 and detailed in the supplementary Tables 1 to 8. Briefly, our predictive model showed a promising performance in classifying glioma grades and types on the TCGA dataset (Fig. 3a, c, e, and g) (Supplementary Tables 1, 3, 5, and 7). Additionally, we achieved satisfactory results in predicting glioma grades in our cohort (Fig. 3b and f) (Supplementary Tables 2 and 6). However, the performance for grading oligodendrogliomas and classifying glioma types requires further improvement (Fig. 3d and h) (Supplementary Tables 4 and 8).
Classification performance of the weakly supervised prediction model. ROC curve of prediction of glioma histopathology validated on the internal test set of TCGA (a, c, e, and g), and the external test set of WCH (b, d, f, and h) using the weakly supervised deep learning model.
We selected and presented representative heatmaps of HE images of each tumor type from five patients in the TCGA dataset. Magnified heatmaps illustrate how the deep learning model identifies specific and critical pathological features (Fig. 4a–e). In the case of anaplastic astrocytoma (IDH-mutant) (Fig. 4b) and anaplastic oligodendroglioma (IDH mutant and 1p/19 codeletion) (Fig. 4d), the model prominently highlighted regions of pathological microvascular proliferation and marked increases in cellularity with heterogeneity, in contrast to the astrocytoma (IDH-mutant, grade 2) (Fig. 4a) and oligodendroglioma (IDH mutant and 1p/19 codeletion, grade 2) (Fig. 4c). Furthermore, the heatmap generated by the model accurately identified the highest-risk region characterized by palisading necrosis and dense nuclei within the core area of glioblastoma (Fig. 4e). These examples visually depict the risk features associated with different glioma types and may enhance and inform pathological practice.
Representative heatmap outputs for glioma diagnosis generated by the weakly supervised deep-learning model. (a) Astrocytoma, IDH-mutant, WHO grade 2. (b) Anaplastic Astrocytoma, IDH-mutant, WHO grade 3. (c) Oligodendroglioma, IDH-mutant and 1p/19q codeletion, WHO grade 2. (d) Anaplastic Oligodendroglioma, IDH-mutant and 1p/19q codeletion, WHO grade 3. (e) Glioblastoma, IDH-wildtype, WHO grade 4. Magnification of the primary HEs and their corresponding heatmaps were 10X. Magnification of the enlarged heatmaps of the right column was 100X.
IDH mutation status is regarded as the primary decisive biomarker for distinguishing glioblastomas from other diffuse gliomas (Fig. 5a). The deep learning model differentiated IDH-mutant WSIs from IDH-wildtype in the TCGA dataset with a mean AUC of 0.9488 (Fig. 5b) (Supplementary Table 9). The confusion matrix revealed an accuracy of 91.8% for identifying IDH-wildtype and 86.1% for IDH mutant gliomas in the TCGA dataset, respectively (Fig. 5c).
IDH status prediction of the weakly supervised prediction model. (a) Representative HE images of anaplastic astrocytoma, IDH mutant (AA, IDH-mutant), and glioblastoma, IDH wildtype (GBM, IDH-wildtype). Magnification, 100X. (b) ROC curve of prediction of the IDH biomarker employing the TCGA dataset. (c) Confusion matrix showing the performance of the model in predicting IDH mutation status in the TCGA dataset.
With the publication of the fifth edition of the CNS tumor classification, molecular pathology has emerged as the cornerstone of glioma therapy2. However, histopathological morphology identification remains essential as the primary step in glioma diagnosis for classifying gliomas. Undoubtedly, these factors increase the workload for pathologists. To enhance the diagnostic efficiency and accuracy of gliomas in clinical practice, computer-aided diagnosis using AI based on the DCNN is gaining significant attention7,22. Building on a previously reported weakly supervised deep learning model19, we conducted an AI-assisted predicting analysis for gliomas using both the TCGA and WCH datasets. In this study, our prediction model accurately distinguishes the grades and origins of all gliomas. In addition, our model can further successfully identify IDH mutant. Furthermore, the diagnostic heatmap generated by the model aligns closely with the diagnostic process of pathologists, highlighting representative risk features. Therefore, we demonstrate that the weakly supervised deep learning model could serve as a useful aid for the pathological diagnosis of gliomas.
To ensure timely therapeutic intervention for patients, pathologists need to diagnose brain tumors promptly after tumor resection. As glioma is the most common primary malignant brain tumor1, identifying WHO grades or molecular markers of gliomas is a top priority for neuropathologists. Our research revealed that the diagnostic accuracy for distinguishing astrocytoma and oligodendroglioma grades of the weakly supervised deep learning model was about 0.98 and 0.86 on the TCGA dataset.
Importantly, these accuracies also reached 0.90 and 0.74 in our cohort. A study reported that a whole slide imaging-based deep learning model identified intracranial germinoma, astrocytoma, and oligodendroglioma with internal and external validation accuracies of 95.3% and 76.9%, respectively15. Although the high accuracy of our study for astrocytoma aligned with the aforementioned research, the internal and external accuracies for oligodendrogliomas of that research were only 83.3% and 72.2% 16, indicating that the performance of our model in identifying oligodendroglioma could still be improved. Notably, our model could predict the WHO grades of all diffuse gliomas, with diagnostic accuracies for identifying gliomas (WHO grade 2 and 3) and glioblastomas reaching 0.99 and 0.95 in the external validation set of TCGA and WCH, respectively. Recently, a weakly supervised learning model achieved an accuracy of 0.94 in a classification task of nine brain tumor types on an independent dataset, including oligodendrogliomas, astrocytomas, ependymoma, lymphoma, and metastasis21. Additionally, a vision transformer-based weakly supervised histopathological image analysis not only predicted histopathological subtypes of eight brain tumors but also demonstrated high accuracy in identifying three glioma molecular markers: IDH1 mutation, P53 mutation, and MGMT methylation16. These researches provided great convenience for pathologists in diagnosing a wide range of brain tumors. Our study also suggested that the weakly supervised learning model has reliable predictive power for identifying IDH mutations in gliomas.
Traditionally, deep learning models analyzing tissue slides have relied on manual ROI selection or risk features labeling of experienced pathologists. It hinders the clinical application of computational-aided diagnosis7,8,22,23,24. Although supervised deep learning has already yielded promising results on small datasets, its clinical application remains uncertain due to the substantial variability among independent samples6,25. A pioneering large-scale study confirmed that a weakly supervised deep learning model achieved high accuracy on the CAMELYON16 test set for detecting metastatic breast cancer, comparable to the results of the original supervised deep learning model6. It suggested that a supervised deep learning model trained on small datasets and with patch-level annotations may not generalize well in real-world practice. In contrast, the weakly supervised algorithm can process large and diverse datasets without requiring additional management by pathologists, warranting further in-depth investigation of this new method. As for the diagnostic accuracy of weakly supervised learning models for brain tumors, accumulating evidence has demonstrated their efficiency in identifying subtypes and grades of gliomas, and other brain tumors15,16,17,21. Even so, the present study, based on our dataset, offers additional evidence that the robust weakly supervised learning model can accurately diagnose grades and a molecular marker of gliomas at the slide level without expert supervision. Furthermore, future studies validating the accuracy and efficiency of weakly supervised AI-assisted pathological classification should be conducted across multiple institutions.
Our study has several limitations. The results showed limited power for distinguishing both grades of oligodendrogliomas and the origin of astrocytoma and oligodendroglioma in our dataset (Fig. 3d and h). We used only 472 WSIs of our center for external validation, a number significantly lower than the TCGA dataset. Future studies should expand this to include more WSIs from multiple medical centers to comprehensively validate the model’s diagnostic accuracy. Molecular diagnosis is a more vital and complicated process in classifying gliomas. We validated a promising prediction value of the weakly supervised deep learning model for IDH mutation on the TCGA dataset. Unfortunately, we were unable to conduct the same analysis with our data due to the limited size of our IDH status database. Thus, it remains to be demonstrated whether the deep learning model can be applied to classifying IDH mutation and other molecular statuses in our center following dataset expansion. We also acknowledge that future work should address the diagnosis of tumor tissue sections from distinct anatomical locations to overcome the challenges posed by intratumoral heterogeneity. Finally, we consider it essential to refine the algorithms of the deep learning model to enhance its intelligence and diagnostic accuracy.
In summary, we utilized a weakly supervised deep learning model with high automation and reasonable efficiency for the pathological diagnosis of gliomas. This model should be applied to assist in the pathological diagnosis of gliomas in the future, enabling pathologists to achieve higher accuracy and efficiency in their diagnoses and, in turn, providing patients with timely post-operative treatment.
The present study retrospectively collected 472 HE staining slides of glioma tissues from WCH of Sichuan University and selected 1604 HE staining slides of gliomas from the public TCGA. All diagnoses of WSIs were evaluated by two senior pathologists of the Department of Pathology of WCH. Our study was performed according to the principles of the Declaration of Helsinki. Our study was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University (No.2021.1319) and written informed consents were attained from patients or their legal guardians. The inclusion criteria were as follows: (I) Patients were diagnosed with gliomas based on the histological and molecular biomarkers according to the fifth edition of the 2021 classification of CNS tumors. (II) Available HE slides are suitable for acquiring high-quality WSIs. Exclusions were as follows: I. Partial regions of HE staining from both TCGA and WCH datasets were damaged, contaminated, or blurry. For WSIs from the TCGA cohort, we revised the diagnosis of gliomas before 2021 based on the fifth edition of 20212.
WSIs of HE slides (Magnification 10x) from the TCGA dataset were scanned using the Aperio Imagescope-Pathology Slide Viewing Software. The representative WSIs (Magnification 10x) obtained from our center were scanned by the automatic digital scanner of Hamamatsu NanoZoomer-SQ (C13140, Hamamatsu, Japan). We took a three-step image preprocessing method to convert the original WSI into segmentations. Preprocessing used the programming language Python version 3.7.4 and Jupyter Lab (https://jupyter.org). Details are presented in Fig. 1: I. All procedures relating to programming of these steps operated in the cloud serves of Hua Wei (http://www.huaweicloud.com/) utilizing the operating system of Ubuntu 16.04 server 64bit. Firstly, the OpenSlide (Version 3.4.1) was used to read WSIs and fulfill data vectorization26. Secondly, images of WSIs were segmented into non-overlapping patches at a resolution of 512 × 512 pixels by the DeepZoom module, and each patch with more than 50% of the background was removed by the Grab cut algorithm27,28. Then, color standardization of all heterogeneous WSIs was performed through the Reinhard method29.
To develop a weakly supervised deep learning model, all WSIs from the TCGA dataset were allocated into the training and testing, and internal validating test sets in a proportion of 8:1:1. Figure 1 shows the overview of model development procedures. Based on the approach presented by Lu et al.19, the weakly supervised deep learning model was developed and trained using PyTorch1.3. We used the DCNN of ResNet-50 to obtain high-level visual features of patches. It is difficult and time-consuming to annotate enough specific ROIs on WSIs to develop a DCNN suitable for glioma detection. Therefore, we also utilized transfer learning to optimize high-level visual feature extraction30. All weights of convolutional layers of the ResNet-50 were trained on the ImageNet dataset31. Unlike the classical deep learning model fulfills diagnostic tasks at a patch level, our analysis tries to predict diagnosis at a WSI-level. To design weakly supervised deep learning algorithms that could efficiently tackle WSI images with high-resolution and information content, we used the attention mechanism of deep learning32. We performed dimension reduction for patches to reduce their calculation amount through the full connection layer, and then patches connected with the attention network compiled by the attention layer. The attention network was divided into many classifiers. Finally, we conducted diagnostic classifying and acquired confidence scores by connecting the output of the attention layer with the classifying layer with the Softmax activation function. We further analyzed the external validation set from our institution to obtain the objective prediction value by the weakly supervised deep learning model. Results were also plotted into a confusion matrix to describe the performance of this trained model.
We performed the training procedure with a method called k-fold cross-validation with the following procedure. (1) We split data into k groups. As we used 10-fold cross-validation, thus we split the data into ten groups. (2) Train and test k times: we set aside one group (Group 0) for interval validation and used the remaining groups (Groups 1,2, …8,9) as the training set and testing set in the first round, we termed the fold 0. Next, we set aside Group 1 for interval validation and used the rest (Groups 0, 2, 3…8,9) for training and testing set in the second round, which was termed fold 1. Then, we repeated this process k times (k = 10 in our study) so that every group was to be the internal validation data exactly only once. (3) Averaging the results: we take the results (accuracy and AUC) from each round and calculate the average performance after ten rounds.
To understand the specific contents learned by the deep learning model, visualization of model execution was performed following training of the model. Extract and record the location of scores of K (m, n) of each patch, and transform these scores into 0 to 1. Then, standardized scores were converted to red, green, and blue (RGB), and diverging colormap was used to draw heatmaps of which the higher attention scores meant a higher probability of becoming red, while the lower attention scores represented the color was closer to blue. Finally, we assembled heatmaps of all patches according to previously recorded location and overlaid primary WSIs with corresponding heatmaps after setting the diaphaneity of all assembled heatmaps to 50%, which made it possible to observe histopathological sections accompanied with attention scores. The regions of top scores of WSIs with the strongest confidence denoted correctly classified risk features.
Data were divided into the k sets of which k-1 for training and 1 for cross validation. To validate the reliability of the model, we used the k-fold cross-validation technique to evaluate the accuracy through training and testing divided data. To appraise the accuracy and specificity of the prediction model, the ROC curve and AUC were calculated in Python with the Matplotlib package.
The TCGA datasets are publicly available (https://portal.gdc.cancer.gov/). Our hospital’s data are presently unavailable due to hospital requirements governing privacy protection but are available from the corresponding author on reasonable request.
Ostrom, Q. T. et al. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2015–2019. Neuro-oncology 24, v1–v95 (2022).
Louis, D. N. et al. The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro-oncology 23, 1231–1251 (2021).
Louis, D. N. et al. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 131, 803–820 (2016).
Article PubMed MATH Google Scholar
Holdhoff, M. et al. The consistency of neuropathological diagnoses in patients undergoing surgery for suspected recurrence of glioblastoma. J. Neurooncol. 141, 347–354 (2019).
Article CAS PubMed Google Scholar
Louis, D. N. et al. Computational pathology: A path ahead. Arch. Pathol. Lab. Med. 140, 41–50 (2016).
Article PubMed MATH Google Scholar
Campanella, G. et al. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat. Med. 25, 1301–1309 (2019).
Article CAS PubMed PubMed Central MATH Google Scholar
Mobadersany, P. et al. Predicting cancer outcomes from histology and genomics using convolutional networks. Proc. Natl. Acad. Sci. 115, E2970–E2979 (2018).
Kather, J. N. et al. Predicting survival from colorectal cancer histology slides using deep learning: A retrospective multicenter study. PLoS Med. 16, e1002730 (2019).
Article PubMed PubMed Central Google Scholar
Veldhuizen, G. P. et al. Deep learning-based subtyping of gastric cancer histology predicts clinical outcome: A multi-institutional retrospective study. Gastric Cancer, 1–13 (2023).
Barker, J., Hoogi, A., Depeursinge, A. & Rubin, D. L. Automated classification of brain tumor type in whole-slide digital pathology images using local representative tiles. Med. Image. Anal. 30, 60–71 (2016).
Article PubMed Google Scholar
Zadeh Shirazi, A. et al. A deep convolutional neural network for segmentation of whole-slide pathology images identifies novel tumour cell-perivascular niche interactions that are associated with poor survival in glioblastoma. Br. J. Cancer. 125, 337–350 (2021).
Article PubMed PubMed Central MATH Google Scholar
Ertosun, M. G. & Rubin, D. L. in AMIA annual symposium proceedings. 1899 (American Medical Informatics Association).
Im, S. et al. Classification of diffuse glioma subtype from clinical-grade pathological images using deep transfer learning. Sensors 21, 3500 (2021).
Article ADS PubMed PubMed Central MATH Google Scholar
Jiang, S., Zanazzi, G. J. & Hassanpour, S. Predicting prognosis and IDH mutation status for patients with lower-grade gliomas using whole slide images. Sci. Rep. 11, 16849 (2021).
Article ADS CAS PubMed PubMed Central Google Scholar
Shi, L. et al. Contribution of whole slide imaging-based deep learning in the assessment of intraoperative and postoperative sections in neuropathology. Brain Pathol., e13160 (2023).
Li, Z. et al. Vision transformer-based weakly supervised histopathological image analysis of primary brain tumors. iScience 26 (2023).
Hsu, W. W. et al. A weakly supervised deep learning-based method for glioma subtype classification using WSI and mpMRIs. Sci. Rep. 12, 6111 (2022).
Article CAS PubMed PubMed Central MATH Google Scholar
Kanavati, F. et al. Weakly-supervised learning for lung carcinoma classification using deep learning. Sci. Rep. 10, 9297 (2020).
Article ADS CAS PubMed PubMed Central MATH Google Scholar
Lu, M. Y. et al. Data-efficient and weakly supervised computational pathology on whole-slide images. Nat. Biomedical Eng. 5, 555–570 (2021).
Article MATH Google Scholar
Lu, M. Y. et al. AI-based pathology predicts origins for cancers of unknown primary. Nature 594, 106–110 (2021).
Article ADS CAS PubMed MATH Google Scholar
Ma, Y. et al. Histopathological auxiliary system for brain tumour (HAS-Bt) based on weakly supervised learning using a WHO CNS5-style pipeline. J. Neurooncol., 1–12 (2023).
Jin, L. et al. Artificial intelligence neuropathologist for glioma classification using deep learning on hematoxylin and eosin stained slide images and molecular markers. Neuro-oncology 23, 44–52 (2021).
Article CAS PubMed MATH Google Scholar
Das, K., Karri, S. P. K., Roy, A. G., Chatterjee, J. & Sheet, D. in IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017). 1024–1027 (IEEE, 2017).
Ehteshami Bejnordi, B. et al. Using deep convolutional neural networks to identify and classify tumor-associated stroma in diagnostic breast biopsies. Mod. Pathol. 31, 1502–1512 (2018).
Article PubMed MATH Google Scholar
Wang, D., Khosla, A., Gargeya, R., Irshad, H. & Beck, A. H. Deep learning for identifying metastatic breast cancer. arXiv preprint https://arxiv.org/abs/1606.05718 (2016).
Goode, A., Gilbert, B., Harkes, J., Jukic, D. & Satyanarayanan, M. OpenSlide: A vendor-neutral software foundation for digital pathology. J. Pathol. Inf. 4, 27 (2013).
Article Google Scholar
Kwatra, V., Schödl, A., Essa, I., Turk, G. & Bobick, A. Graphcut textures: Image and video synthesis using graph cuts. Acm Trans. Graphics (tog). 22, 277–286 (2003).
Article Google Scholar
Rother, C., Kolmogorov, V. & Blake, A. GrabCut interactive foreground extraction using iterated graph cuts. ACM Trans. Graphics (TOG). 23, 309–314 (2004).
Article MATH Google Scholar
Mesko, B. Vol. 2 239–241 (Taylor & Francis, 2017).
Ribani, R. & Marengoni, M. in 2019 32nd SIBGRAPI conference on graphics, patterns and images tutorials (SIBGRAPI-T). 47–57 (IEEE).
Deng, J. et al. in 2009 IEEE conference on computer vision and pattern recognition. 248–255 (Ieee).
Vaswani, A. et al. Attention is all you need. Adv. Neural. Inf. Process. Syst. 30 (2017).
Download references
This work was supported by grants from the internal research funds in West China Hospital of Sichuan University (19HXCX009), the Sichuan Science and Technology Program (2023YFQ0002), the National Key R&D Program of China (2022ZD0116100), the National Natural Science Foundation of China (62276055), the Sichuan Science and Technology Program (2023YFG0288).
Mingrong Zuo, Xiang Xing and Linmao Zheng contributed equally to this work.
Department of Neurosurgery, West China Hospital, Sichuan University, 37 Guoxue Avenue, Chengdu, 610041, People’s Republic of China
Mingrong Zuo, Xiang Xing, Yunbo Yuan, Siliang Chen, Yuan Yang, Qing Mao & Yanhui Liu
Department of Pediatric Neurosurgery, Key Laboratory of Birth Defects and Related Diseases of Women and Children of Ministry of Education, West China Second University Hospital, Sichuan University, Chengdu, 610041, China
Mingrong Zuo
Department of Pathology, West China Hospital, Sichuan University, 37 Guoxue Avenue, Chengdu, 610041, People’s Republic of China
Linmao Zheng, Tianping Yu & Ni Chen
School of Information and Software Engineering, University of Electronic Science and Technology of China, Chengdu, 610054, People’s Republic of China
Hao Wang & Yongbin Yu
Department of Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China
ShuXin Zhang
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
You can also search for this author in PubMed Google Scholar
M.R. Zuo, X. Xing, L.M. Zheng, and H. Wang collected all the data; Y.H. Liu, N. Chen, and Y.B. Yu conceived the study; L.M. Zheng, T.P. Yu, and N. Chen conducted pathological diagnosis; M.R. Zuo, X. Xing, L.M. Zheng, and H. Wang, Y.B. Yuan, S.L. Chen, S.X. Zhang processed data and performed the analysis; M.R. Zuo, X. Xing, and L.M. Zheng drafted the manuscript and all authors revised the final edition.
Correspondence to Ni Chen or Yanhui Liu.
The authors declare no competing interests.
Our study was performed according to the principles of the Declaration of Helsinki. Our study was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University (No.2021.1319) and written informed consents were attained from patients or their legal guardians.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Below is the link to the electronic supplementary material.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Reprints and permissions
Zuo, M., Xing, X., Zheng, L. et al. Weakly supervised deep learning-based classification for histopathology of gliomas: a single center experience. Sci Rep 15, 265 (2025). https://doi.org/10.1038/s41598-024-84238-x
Download citation
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-84238-x
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Advertisement
© 2025 Springer Nature Limited
Sign up for the Nature Briefing: Cancer newsletter — what matters in cancer research, free to your inbox weekly.


More Stories
How One Alum Helped Build a Community of Internet Leaders
The Tribal Broadband Bootcamps Celebrate Their Five-Year Anniversary
Adaptability and Resilience: Q&A with New Board Chair Brian Haberman